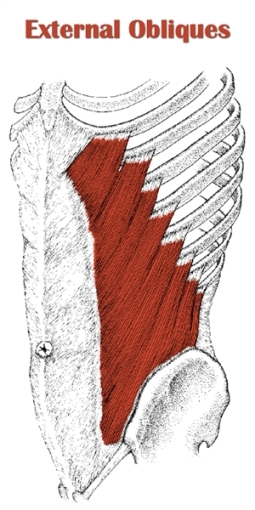
 The external oblique (L. externus, external ; obliquus, oblique.) is a broad, flat sheet of muscle on either side of the abs.
The external oblique (L. externus, external ; obliquus, oblique.) is a broad, flat sheet of muscle on either side of the abs.
It is named after its location (external to the internal oblique) and its fiber direction (oblique relative to the midline of the body).
It is the prime mover in spinal rotation, and it has a significant role in spinal lateral flexion.
Notably, it also helps posteriorly tilt the pelvis and assists in respiration by compressing the abdominal wall during forced expiration.
The external and internal obliques, together known as the obliques, work in tandem to perform the same actions. The main difference is that the external obliques are opposite-side rotators and the internal obliques are same-side rotators (e.g. rotation to the left involves the right external oblique and left internal oblique).
It is part of the anterolateral abdominal wall, lying superficial to to the internal oblique and transversus abdominis.
It is almost completely visible from the surface of the physique, with only its posterior and superior portions lying deep to the serratus anterior and latissimus dorsi.
It originates from the lower eight ribs and inserts on the front of the pelvis and external oblique aponeurosis.
It has parallel-orientated fibers that run inferior and anterior from origin to insertion, and form a flat muscle architecture.
When sufficiently developed, the external obliques can make an impressive aesthetic impact on the physique at low body fat percentages. Its visual effect is most noticeable where the it interdigitates with the serratus anterior as well as right above the pelvis.
Table of Contents
Also Called
- Side abs
- Outer oblique
Origin, Insertion, Action & Nerve Supply
| Muscle | External Oblique |
|---|---|
| Origin | External surface of the ribs 5-12 |
| Insertion |
|
| Action | Unilateral contraction:
Bilateral contraction:
|
| Nerve Supply |
|
Exercises:
Note: I have only included exercises that target the external obliques directly. These are the same exercises for the internal obliques. For exercises that train the obliques indirectly, see abdominal exercises.
Barbell Exercises:
- Standing side bend
- Seated side bend
- Standing twist
- Seated twist
Dumbbell Exercises:
- Standing side bend
- Seated side bend
- Roman chair side bend
- Standing overhead side bend
- Russian twist
- Russian twist on exercise ball
- Hanging twisting knee raise DB between ankles
- Captains chair twisting knee raise DB between ankles
Cable Exercises:
- Standing side bend
- Standing side crunch
- Seated side crunch
- Standing overhead side bend
- Standing twist
- Seated twist
- Kneeling twist
- Half-Kneeling twist
- Standing chop
- Kneeling chop
- Half-kneeling chop
- Standing lift
- Kneeling lift
- Half-kneeling lift
- Standing twisting crunch
- Kneeling twisting crunch
- Russian twist on exercise ball
Machine Exercises:
- Standing side bend
- Seated side bend
- Seated side crunch
- Seated twist
- Kneeling twist
- Lying twist
Weighted Exercises:
- Roman chair side bend
- Side crunch
- Standing overhead side bend
- Twisting crunch
- Decline twisting crunch
- Twisting sit up
- Decline twisting sit up
- Russian twist
- Russian twist on exercise ball
Bodyweight Exercises:
- Roman chair side bend
- Side crunch
- Side bridge
- Incline side bridge
- Twisting crunch
- Decline twisting crunch
- Twisting sit up
- Decline twisting sit up
- Russian twist
- Russian twist on exercise ball
- Lying leg twist
- Hanging twisting knee raise
- Captains chair twisting knee raise
Isometric Exercises:
- Side plank
- Feet elevated side plank
Stretches & Myofascial Release Techniques:
Stretches
- Standing oblique stretch
- Lying bent leg oblique stretch
- Seated bent leg oblique stretch
Self Myofascial Release Techniques
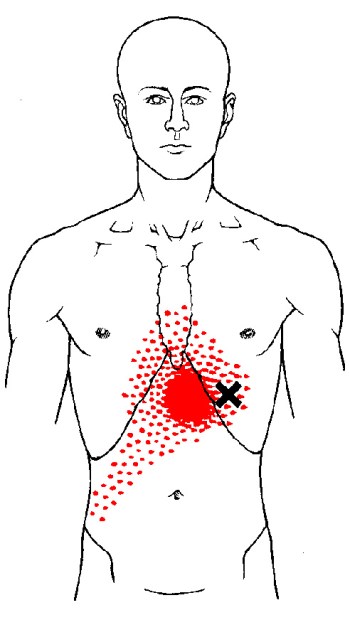
When using these techniques, give special attention to the common trigger points shown in the image below.
Tool
- Backnobber II
- Posture ball
- Foam roller
Common Issues:
- Inhibited/Lengthened External Obliques: The external obliques are inhibited and excessively lengthened in people with lower crossed syndrome (LCS). The anterior pelvic tilt that is a hallmark of LCS causes the lower attachment on the pelvis to move down and away from the upper attachment on the ribs, thereby stretching the muscle out and inhibiting it. This simultaneously facilitates the hip flexors and lumbar erectors, both of which reciprocally inhibit the external obliques when overactive. Since the external oblique plays a role in proper positioning of the pelvis and lumbar spine, its inhibition/lengthening can do lead to poor core stability, which increases the likelihood of lower back injury. Also, sports hernias may occur if the external obliques and lower abdominals are weak relative to hip adductors.
- Inhibited/lengthened external obliques can also contribute to swayback posture. Although you’d think the external obliques would be short in this posture because of the posterior pelvic tilt in this type of postural dysfunction. However, it is put in a lengthened position because the hips are shifted forward relative to the ribcage.
- Overactive/Short External Obliques: The external obliques, particularly the anterior fibers, are overactive and short in people with upper crossed syndrome (UCS). The excessive thoracic kyphosis that characterises UCS positions the ribcage closer to the pelvis, which shortens the distance between upper and lower attachments of the external oblique, and facilitates the muscle. Overactive/short external obliques can indirectly increase the chance of shoulder injury. This is because they contribute to increased thoracic kyphosis, which limits overhead range of motion and reduces shoulder/scapular stability.
Note: Unilateral inhibition/lengthening or overactivity/shortening of the external oblique (and internal oblique) can cause the torso to bend slightly to the side.
- Example: If the right external and internal obliques are inhibited/lengthened, the torso will bend laterally to the left; if the right external and internal obliques are overactive/short, the torso will bend laterally to the right.
Also, if one external oblique is inhibited/lengthened and the internal oblique on the opposite side is also inhibited/lengthened, then the torso will bend laterally and rotate toward the side of the inhibited internal oblique.
- Example: If the left external oblique and right internal oblique are inhibited/lengthened, the torso will bend to the right and rotate forward on the right.
Training Notes:
-
- If you have inhibited and excessively lengthened external obliques, consider the following:
- Increase volume and frequency on oblique exercises and abdominal exercises.
- Release and stretch the hip flexors and lumbar erectors on a daily basis. Be gentle when stretching your lower back.
- Avoid sitting or standing in excessive anterior pelvic tilt with your lower back excessively arched.
- The above points should help get you started. However, if lower crossed syndrome is at the root of your inner obliques dysfunction, you need to address it for a complete solution. Refer to my guide on how to fix lower crossed syndrome (article coming soon).
- Note: If you have swayback posture, which is less common than LCS, then some of the information in the above bullet points won’t apply. For example, it’s usually recommended to limit ab exercises; and to focus on strengthening the hip flexors/lumbar erectors instead of releasing/stretching them. See swayback posture (article coming soon) for details.
- If you have overactive and short external obliques, consider the following:
- Reduce training volume and training frequency on oblique exercises.
- Reduce training volume and training frequency on ab exercises that involve bringing your rib cage towards your pelvis.
- Increase training volume and training frequency on ab exercises that involve bringing your pelvis closer to your ribcage (i.e. lower ab exercises like the reverse crunch) and isometric ab exercises (e.g. planks).
- Release and stretch your obliques and upper abdominals on a daily basis.
- Avoid postures where you’re hunched over.
- Upper crossed syndrome is often an underlying cause of overactive/short external obliques, which must be addressed to permanently fix the problem. Assuming you have UCS, refer to how to fix upper crossed syndrome (article coming soon).
- If you have a unilateral dysfunction of the obliques (i.e. same-side external/internal oblique inhibition or overactivity; or external oblique inhibition on one side with internal oblique inhibition on opposite side), consider the following:
- Any of these unilateral dysfunctions may be a sign that some form of scoliosis is present or developing – or they may not be. It could be something completely different, such as a true leg length discrepancy, or simply a muscle imbalance with no bone structure abnormalities involved. If you think you may be developing scoliosis, especially if you’re young, see your doctor to find out.
- If you have inhibited and excessively lengthened external obliques, consider the following:
- For general oblique training guidelines and techniques tips, see below. (Note: This applies both internal and external obliques, since you can’t train them separately.)
- If you are worried about your waist becoming too thick from external oblique hypertrophy, consider avoiding or otherwise restricting direct oblique training. I personally believe it’s pretty difficult to build up your obliques to the point that they have a negative impact on your V-taper and overall aesthetics, but it’s certainly possible for some people given enough time. To avoid this, you could skip oblique training altogether. However, I think the best compromise is to limit training volume and use light weight. This way, you can strengthen and condition the obliques to an extent, but minimize unwanted muscle gain.
- Train obliques 1-3 times per week. Use resistance that allows you do 5-20 reps per set. Perform 3-6 sets per session to start with.
- If you want to minimize mass gains, stick to the 12-15+ rep range for all sets. And limit training to just 1 or 2 days per week, doing fewer sets per session (i.e. 3-4 sets, 1-2 times per week).
- If you want to maximize strength and aren’t concerned with the extra hypertrophy that may occur over time, include some heavier sets in the 5-8 rep range. And train more frequently and do a higher number of sets per session (i.e. 5-6 sets, 2-3 times per week)
- Combine abdominal training and obliques training in the same session. This will make your training more efficient and effective, since many oblique exercises indirectly train the abs, and vice versa.
- Avoid training your obliques and abs before doing any major compound movements in your workouts. This will fatigue your core, which decreases your strength/performance and increases the potential for injury. Instead, implement either of the following strategies:
- Train the obliques and abs at the end of your workout.
- Or, dedicate a separate workout session to training them just core work. If you go with this option, you can also add in some work for other small muscle groups that may not get enough attention on your main training days (e.g. calves, forearms).

LOVING your blog thank you alex,incredibly informative. I notice the images related to some descriptions of exercises and releases in the tables above are missing – any chance you can add them in soon? Tia
Thanks, Heather! It’s on my to-do list. Unfortunately, it’s a long to-do list it’ll be at least a few months before I get back to those images. When I eventually do these updates, I’ll let everyone on my newsletter list know about it–so be sure to sign up if you’re not already. You can sign up here: https://www.kingofthegym.com/myx8/
I love your posts!!
If you don’t mind, Can I know a book by reference?
Dude, you’re a lifesaver! Your posts are so informative and provide a great help for me to learn about the muscles I want to focus my future workouts on. Thanks bunches.
“It is part of the anterolateral abdominal wall, lying superficial to to the external oblique and transversus abdominis.”
I think you meant “internal oblique” not “external?”
Just letting you know 🙂
Thanks for catching that mistake, Courtney! Just updated it.
Hello! What if I have both, lower and upper cross syndrome at the same time?
That’s not uncommon. You’ll just have to focus on fixing both together. Exercises and stretches/myofascial release help (study the various anatomy pages to know which ones to try). However, the one KEY thing you have to focus on while doing any routine, is to correct the bad postural habits that contribute to UCS & LCS throughout the day. Habit change is hard, and takes a while, but it works!