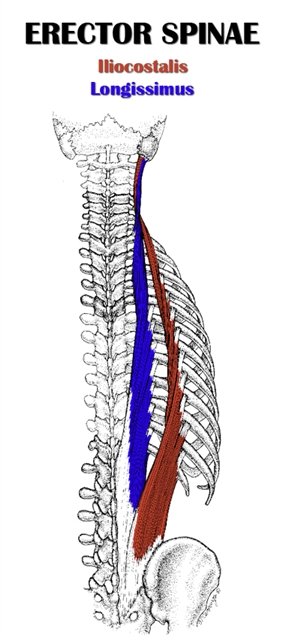
 The erector spinae (erigere, to erect ; spina, spine.) consists of three long, thin muscle groups running vertically up each side of the vertebral column: the iliocostalis, longissimus and spinalis.
The erector spinae (erigere, to erect ; spina, spine.) consists of three long, thin muscle groups running vertically up each side of the vertebral column: the iliocostalis, longissimus and spinalis.
These muscles act on different segments of the vertebral column (i.e. lumbar, thoracic, cervical). Collectively, they are the prime movers in spinal extension and spinal lateral flexion.
The iliocostalis is the lateral muscle group, the longissimus is the intermediate muscle group and the spinalis is the medial muscle group.
Each of these muscle groups can be divided into three segments, making a total of nine individual muscles that constitute the erector spinae.
Classified as intermediate intrinsic back muscles, the erector spinae lie deep to the splenius muscles, serratus posterior superior and inferior, and all the superficial extrinsic back muscles. They lie superficial to the transversospinales muscles and the minor deep back muscles.
The erector spinae muscles arise from different points on the pelvic and lower back regions, vertebral column or ribs. They have a parallel-oriented fibers, which run superiorly along the spine, and insert on the vertebrae, ribs or skull.
Note: I’ll provide a much more detailed description of origin and insertion attachments, below.
Remember, there are nine erector spinae muscles with attachment points at different locations along the spine. So the different muscles control the different regions of the spine.
- The muscles that extend the lumbar spine are called lumbar erectors, or lower erectors.
- The muscles in charge of extending the thoracic spine are thoracic erectors, or upper erectors.
- The muscles that extend the cervical spine are called cervical erectors.
While sources on muscle architecture are scarce, the ones I found classify the erector spinae as having a parallel fiber orientation and a strap-like shape.
Table of Contents
Also Called
- Spinal erectors
- Spinal extensors
- Extensor spinae
- Sacrospinalis
Origin, Insertion, Action & Nerve Supply
| Muscle | Iliocostalis cervicis | Iliocostalis thoracis | Iliocostalis lumborum | Longissimus capitis | Longissimus cervicis | Longissimus thoracis | Spinalis capitis* | Spinalis cervicis | Spinalis thoracis |
|---|---|---|---|---|---|---|---|---|---|
| Origin | Ribs 3-7 | Ribs 1-6 |
|
|
Transverse processes of T1-T6 |
|
Lateral surface of spinous process of C7 | Spinous processes of C5-T2 | Lateral surfaces of spinous processes of lower thoracic and upper lumbar vertebrae (T10-L3) |
| Insertion | Transverse processes of C4-C6 | Ribs 7-12 |
|
Mastoid process of temporal bone | Transverse processes of C2-C5 |
|
Between the superior and inferior nuchal lines of the occipital bone, toward the median nuchal line | Spinous processes of C2-C5 | Lateral surfaces of spinous processes of thoracic vertebrae (T2-T8) |
| Action | Unilateral contraction:
Bilateral contraction:
|
Unilateral contraction:
Bilateral contraction:
|
Unilateral contraction:
Bilateral contraction:
|
Unilateral contraction:
Bilateral contraction:
|
Unilateral contraction:
Bilateral contraction:
|
Unilateral contraction:
Bilateral contraction:
|
Unilateral contraction:
Bilateral contraction:
|
Unilateral contraction:
Bilateral contraction:
|
Unilateral contraction:
Bilateral contraction:
|
| Nerve Supply | Posterior rami of cervical/thoracic spinal nerves | Posterior rami of upper thoracic/lower cervical spinal nerve | Posterior rami of lower thoracic/upper lumbar spinal nerves | Posterior rami of lower cervical spinal nerves | Posterior rami of cervical/upper thoracic spinal nerves | Posterior rami of lumbar/lower thoracic spinal nerves | Posterior rami of cervical spinal nerves | Posterior rami of upper thoracic/lower cervical spinal nerves | Posterior rami of upper thoracic/lower cervical spinal nerves |
* The spinalis capitis is often so poorly distinguished that it is usually considered to be more of an extension of the semispinalis capitis.
Exercises:
Note #1: In the exercise lists in the following sections, some exercises emphasize the lower spinal erectors (lumbar erectors) while others emphasize the upper spinal erectors (thoracic erectors). Here are some general guidelines on how the most common types of spinal erector exercises target the erectors:
- Deadlifts (all variations) emphasize the lower erectors; the upper erectors still get a significant workout.
- Good mornings (non-round back variations) target the lower erectors.
- Good mornings (round back and seated variations) hit the upper erectors more, but the lower erectors still get worked.
- Upper back good mornings target the upper erectors.
- Using the safety squat bar on any good morning variation will increase the involvement of the upper erectors.
- Rows (bent over variations) emphasize the upper erectors; the lower erectors still get a significant workout.
- Rows (non-bent over variations) target the upper erectors.
- Back extensions, hyperextensions and pull throughs target the lower erectors.
Note #2: The lists below don’t include exercises that target the cervical erectors, since they aren’t typically associated with “spinal erector exercises.” To train them, you must use isolation movements. See cervical extension exercises and cervical lateral flexion exercises for examples.
Note #3: All squat exercises significantly, but indirectly work the erectors. Squat variations where the torso is angled more forward (e.g. low bar squat) activate the lower erectors more. Whereas, upper erector activation is increased in squat variations involving a more upright torso (e.g. front squat, goblet squat, high bar squat).
Barbell Exercises:
- Deadlift
- Romanian deadlift (RDL)
- Sumo deadlift
- Stiff leg deadlift
- Trap bar deadlift
- Good morning
- Round back good morning
- Upper back good morning
- Seated good morning
- Back extension
- Hyperextension
- Bent over row
- Underhand bent over row
- Lying row (cambered bar)
- Incline row (cambered bar)
- T-bar row
Dumbbell Exercises:
- Stiff leg deadlift
- One arm row
- Lying row
- Incline row
Cable Exercises:
- Deadlift
- Stiff leg deadlift
- Pull through
- Seated row
- Underhand seated row
- Lying row
- Incline row
Machine Exercises:
- Deadlift
- Stiff leg deadlift
- Bent over row
- Seated row
- Incline row
- T-bar row
Weighted Exercises:
- Back extension
- Hyperextension
Bodyweight Exercises:
- Back extension
- Hyperextension
- Prone cobra
- Superman
- Contralateral superman
- Bird dog
- Contralateral bird dog
- Thoracic extension (foam roller)
- Side lying thoracic rotation
- Quadruped thoracic extension-rotation
- Cat camel
- Squat to Stand
Isometric Exercises:
- Front squat hold
- Prone cobra hold
- Contralateral superman hold
- Bird dog hold
- Contralateral bird dog hold
- Glute bridge
- Reverse plank
Stretches & Myofascial Release Techniques:
Stretches
- Seated lower back stretch
- Squatting lower back stretch
- Floor-seated lower back stretch
- Lying lower back stretch
- Plow stretch
- Cat stretch
- Standing cat stretch
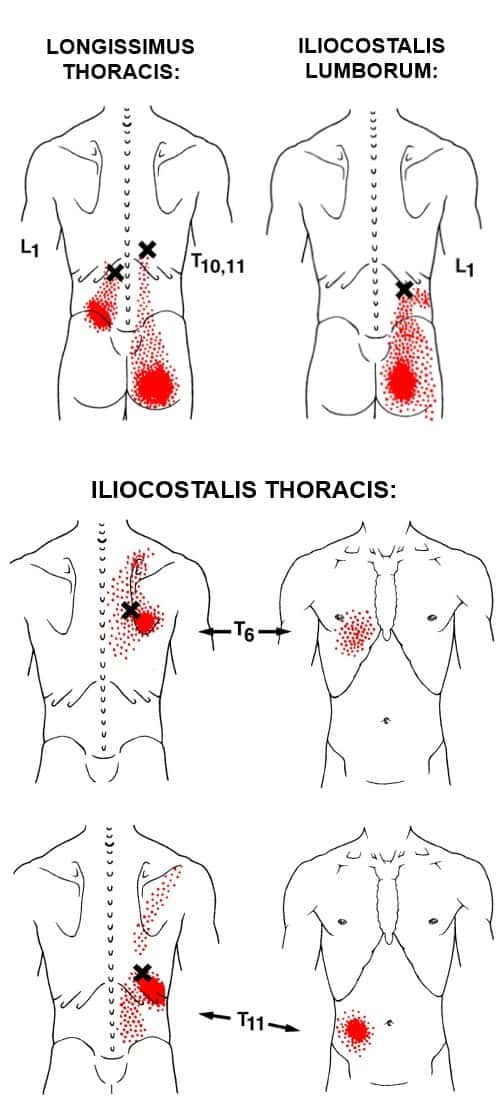
Self Myofascial Release Techniques
When using these techniques, give special attention to the common trigger points shown in the image below.
Tool
- Lacrosse ball
- Double ball
- Backnobber II
- Foam roller
Common Issues:
- Overactive/Short Lower Spinal Erectors: The lumbar spinal erectors are overactive and shortened in individuals with lower crossed syndrome (LCS). The anterior pelvic tilt and excessive lumbar lordosis seen in LCS facilitates these muscles. The overactive lumbar erectors, in turn, reciprocally inhibit the abdominals and pull them into a lengthened state. Overuse of these muscles can cause or contribute to overactivity/shortening of the lower erectors. Specifically, you may default to using the lumbar erectors due to poor technique (e.g. excessive arch or forward lean on squats, torso momentum on rows) or to compensate for weak muscles or poor technique during certain exercises (e.g. weak glutes/abs on deadlifts); or you may have poor postural habits (e.g. standing/sitting with lower back arched). Injuries associated with this issue include lumbar erector strains and bulging or herniated discs.
- Inhibited/Lengthened Upper Spinal Erectors: The thoracic spinal erectors are inhibited and excessively lengthened in those with upper crossed syndrome (UCS). The excessive thoracic kyphosis associated with UCS puts the upper erectors in a chronically stretched out position, which causes them to be inhibited (along with the lower traps, scapular retractors and serratus anterior), while the muscles opposite the upper erectors on the front of the body are facilitated (i.e. pec major, pec minor). Factors that may cause or exacerbate thoracic erector inhibition include bad posture (i.e. slouching), and a disproportionate focus on bench press variations compared to row variations/other erector spinae exercises that train the upper erectors. Upper spinal erector inhibition can contribute to subacromial impingement, which can lead to other injuries (e.g. rotator cuff tear, tendinosis/tendonitis, bursitis).
Training Notes:
- If you have overactive and short lower spinal erectors, consider the following:
- Avoid training the lower spinal erectors directly with exercises like the back extension.
- Increase training volume on abdominal and external oblique exercises, as well as on glute and hamstring exercises.
- Release and stretch your lower back and hip flexors on a daily basis.
- Note: when releasing/stretching the lower back, take it slow and easy, since the spine is more vulnerable in flexion).
- Avoid standing or sitting in a posture where your lower back is excessively arched. Maintain a more neutral spine and pelvic position by engaging your glutes and abs. It will be difficult at first, but eventually it’ll become a habit.
- Lower crossed syndrome may be the underlying problem causing your erector spinae dysfunction. See how to fix lower crossed syndrome (article coming soon).
- If you have inhibited and lengthened upper spinal erectors, consider the following:
- Increase your training volume and training frequency on exercises emphasizing the upper spinal erectors.
- For beginners, this means doing more row exercises.
- Experienced lifters should also do more rows. However, it can also benefit adding exercises like the seated good morning, upper back good morning and/or round back good mornings (all preferably done with a safety squat bar).
- Improve your thoracic mobility. I recommend doing thoracic extensions on a foam roller and side-lying thoracic rotations on the floor.
- Reduce training volume on horizontal push exercises (i.e. benching).
- Reduce training volume on ab exercises involving thoracic spinal flexion (e.g. crunches). Focus more on isometric strengthening exercises the abs (e.g. plank variations).
- Release and stretch your pectoralis major and minor on a daily basis, and especially before doing any back training.
- Adopt better postural habits throughout the day, particularly in regards to slouching. Keep your torso upright and your head high when sitting and standing. And try to cut down on sitting in general.
- Upper crossed syndrome is often the root cause of thoracic erector weakness. If this is the case for you, see how to fix upper crossed syndrome (article coming soon).
- Increase your training volume and training frequency on exercises emphasizing the upper spinal erectors.
- For erector spinae training guidelines and tips, see below:
- Avoid going to failure. And, with the exception of rows and low rep deadlift training, only use loads you can lift for at least 5 reps. This is just a general rule, but unless you’re an experienced competitive powerlifter, the risk of back injury probably isn’t worth the reward of pushing yourself to the limit.
- Unless you have some injury that prevents you from doing so, you should include the deadlift in your routine. This is the best full body exercise for working the entire erector spinae.
- Most people will benefit from some isolation training for the lower erectors.
- Choose one exercise. I recommend starting with back extensions or regular barbell good mornings.
- Do about 3 sets of 6-15 reps, 1-2 times per week.
- Put the exercise toward the end of your training session, after any exercises requiring a lot of core strength/stability (i.e. don’t do them before any heavy compound exercise, especially squats and deadlifts).
- As you become very strong on squats (i.e. 400 lbs+), training the upper erectors directly becomes increasingly helpful. This is true whether or not you have excessive kyphosis. These muscles are more likely to give out under such heavy loads. If your upper erectors aren’t able to resist the weight, your thoracic spine will round too much. This causes your weight to shift forward, which leads to poor form, inefficient movement and increased chance of injury. To train your upper erectors, do the following:
- Increase training volume and frequency on row exercises. This applies to beginner and experienced lifters, alike.
- Experienced lifters can also include one or more advanced upper erector movement (i.e. upper back, seated or round back good mornings – all preferably using a safety squat bar).
- Do a thoracic mobility exercises (see above). A couple good ones are thoracic extensions and quadruped thoracic extension-rotations.
- If you’re a beginner or intermediate, you should never round your lower back in any exercise. When the lumbar spine is in flexion (i.e. rounded), your risk of injury increases dramatically. As a relatively inexperienced lifter, you lack the overall strength, core strength and stability, and body awareness, to be able to do round lower back exercises in a (relatively) safe manner. Advanced lifters, especially advanced powerlifters, are better suited to be able to handle exercises that involve rounding the lower back. Even then, it’s not “safe,” and many advanced powerlifters avoid doing exercises that specifically involve rounding their lower back (e.g. stiff leg deadlift, hyperextension). However, on difficult one-rep max deadlifts, they can pretty safely handle any incidental and sometimes necessary lower back rounding that may occur due to form breakdown.
- Note: I personally advise against doing exercises that specifically involve spinal flexion under load, even for advanced lifters. This means avoiding the stiff leg deadlift and hyperextension. You could do the straight-back stiff leg deadlift (or straight-back straight-leg, or RDL) and back extension instead.
- As with rounding the lower back, beginners and intermediate lifters should also avoid rounding the upper back. They’re likely to injure something due to a lack of strength, stability and body awareness. However, advanced lifters, especially advanced powerlifters, can benefit greatly from round upper back exercises (e.g. upper back good morning, round back good morning) with little if any increased injury risk. Additionally, some powerlifters purposely do so-called “round back deadlifts” to be able to lift more on max deadlift attempts. This deadlift modification involves a lot of upper back rounding with little to no lower back rounding. Because advanced powerlifters have such strong erectors and other core muscles, back injuries on this lift are rare.
Related Muscles
- Splenius
- Semispinalis
- Multifides
- Rotatores

Hi there, I read “Maintain a more neutral spine and pelvic position by engaging your glutes and abs [while sitting].” I can only engage both glutes and abs while concentrating on them – as soon as my concentration lapses, so does the engagement.
Do you mean one should be able to sit with both sets of muscles engaged for an extended period of time (say, 15-20 minutes)?
Also – thanks for taking the time to write this article. The information contained is awesome, and has already helped my squat catch up to my deadlift.
Good day.
Can you please suggest me what to do, for my back and neck pain?
I give you a brief description about what happened in past because of which I having pain on my entire back and neck, in 2003 I got a back injury during bowling( I used to play cricket ) some sound came from fy lower back I think where the hip are joint on right side. I was scared if I tell to my parents they not allow to play again, so didn’t tell them and there was no treatment except massage. It was very difficult for me to move my right leg in forward direction. I was just straight all the time. Or lying on the bed. After 2-3 month I got relief from pain.then again I continue to play. It was same like as before no pain. But I was feeling some pain on my shoulder. But I was felling some pain at same area one some 2-3 times in month. And then in around 2013 I started to feel light pain on my lower and uper and neck also al in right side. Then when I got a job I had enough money to visit Dr. By myself ,first I went to a neurologist, I explained him all that and he did MRI and told me that one nerve is pressed I give you some medicine and some exercise it will be fine. I went Fir physiotherapy. It relieved some pain but still there us pain. So now I’m having lover and upper back pain including neck and headache. And I feel there is less blood flow to my private parts and I feel light pain on my right side hip. And my right side leg is getting weak. I feel my body is twisted from waist. And I got small small nodes in my both inner thigh.
Now the situation is like this that I am always disturbed because of this pain. Headache right side, some times I feel like a current. Neck pain right entire back pain hips pain. Feeling very light in scrotum like there is no blood flow , there is now tenderness. Feeling pain in the rightside of my penis where tbe scrotum are joint. right knee is also some times paining.
Can you please suggest what should I do, which doctor should I visit, what type of test I need to do, which type of stretching or exercise are best to relieve the pain.
Thank you very much
Harpal Rawal
Hey Harpal,
I came to this page accidentally when searching for spine’s issue like the one mentioned here by Alex. I think I may be able to guess by the sound of your explanation that you have disc herniation (disc prolapsed). Probably related to L4/L5 and probably T1-3. Check out for word ‘subluxation’, you may then find more info. I am not a doctor but an engineer. I probably can be of further help to you.
Best wishes
Exceptional, total explanation of this region. Thank you for offering this. Tracey
You’re very welcome Tracey. I’m glad you found it so helpful.
As. Weight lifter and an osteopath , all I can say is core first all else will fall into,place . After an accident all my body wanted to do was lift. A far girl in my youth , my body knew the only way I’d survive is lifting . Be wise do yoga too .
Thanks for the comment, Margaretann!