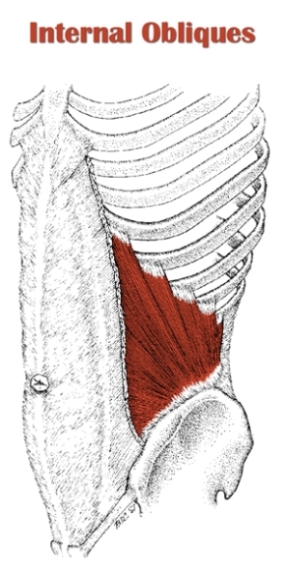
 The internal oblique (L. internus, internal ; obliquus, oblique.) is a flat sheet of muscle on either the side of the lower torso.
The internal oblique (L. internus, internal ; obliquus, oblique.) is a flat sheet of muscle on either the side of the lower torso.
It gets its name from being beneath the external oblique and having an oblique fiber direction relative to the midline.
The most prominent actions of the internal oblique are spinal lateral flexion and spinal rotation.
Notably, it also assists in respiration by compressing the abdominal wall during forced expiration.
The internal and external obliques are collectively referred to as the obliques. They work in tandem to carry out the same movements. The difference is that the internal obliques are same-side rotators, while the external obliques are opposite-side rotators.
So, while the left internal and external obliques both contract for left lateral flexion, the left internal oblique and right external oblique contract for left rotation.
Classified as part of the anterolateral abdominal wall, it is sandwiched between two similarly flat muscles: It lies deep to the external oblique and superficial to the transversus abdominis.
It originates from the lumbar fascia and pelvis. Its parallel-oriented fibers run superior and anterior, inserting on the lower ribs and the internal oblique aponeurosis, forming a flat muscle architecture.
Also Called
- Inner oblique
Origin, Insertion, Action & Nerve Supply
| Muscle | Origin | Insertion | Action | Nerve Supply |
|---|---|---|---|---|
| Internal Oblique |
|
|
Unilateral (one side) contraction:
Bilateral (both sides) contraction:
|
|
Exercises:
Note: These are the same exercises for the external obliques. I have only included exercises that target the obliques directly. For exercises that train them indirectly, see abdominal exercises.
| Type | Name | Picture |
|---|---|---|
| Barbell: |
 Tutorial: N/A
 Tutorial: N/A
 Tutorial: N/A
Tutorial: N/A
|
|
| Dumbbell: |
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
|
|
| Cable: |
|
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
|
| Machine: |
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
|
|
| Weighted: |
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
|
|
| Bodyweight: |
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
|
|
| Isometric: |
Tutorial: N/A
Tutorial: N/A
|
Stretches & Myofascial Release Techniques:
Stretches
| Name | Picture |
|---|---|
|
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
|
Self Myofascial Release Techniques
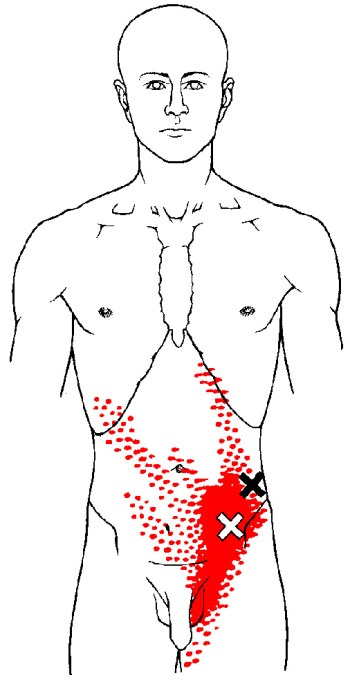
When using these techniques, give special attention to the common trigger points shown in the image below.
| Tool | Picture |
|---|---|
|
Tutorial: N/A
Tutorial: N/A
Tutorial: N/A
|
Common Issues:
- Inhibited/Lengthened Internal Obliques: The internal obliques are inhibited and excessively lengthened in people with lower crossed syndrome (LCS). The excessive lumbar lordosis associated with LCS causes the upper attachment on the ribs to move back and away from the lower attachment on the pelvis, thereby stretching the muscle out and inhibiting it. This simultaneously facilitates the lumbar erectors, which reciprocally inhibit the internal obliques when overactive. The internal oblique is a local stabilizer of the lumbar vertebrae due to its origin on the lumbar fascia. Accordingly, inhibition/lengthening of the muscle can contribute to poor core stability, which in turn increases the risk of lower back injury.
- Overactive/Short Internal Obliques: The internal obliques are overactive and short in those with upper crossed syndrome (UCS). The excessive thoracic kyphosis that characterises UCS causes the ribcage to come down closer to the pelvis. This brings the upper and lower attachments of the internal oblique closer together, allowing the muscle to become facilitated. Since tight internal obliques contribute to increased thoracic kyphosis, it indirectly increases the chance of shoulder injury due to the restriction of overhead mobility associated with excessive kyphosis.
- Overactive/short internal obliques can also contribute swayback posture. They are facilitated by the flat lumbar spine position, since this a more flexed position than the normal lumbar curve.
Note: Unilateral inhibition/lengthening or overactivity/shortening of the internal oblique (and external oblique) can lead to the torso bending slightly to one side.
- Example: If the right internal and external obliques are inhibited/lengthened, the torso will bend laterally to the left; if the right internal and external obliques are overactive/short, the torso will bend laterally to the right.
Also, if the internal oblique on one side is inhibited/lengthened while the external oblique on the opposite side is inhibited/lengthened, the torso will bend laterally and rotate toward the side of the inhibited internal oblique.
- Example: If the right internal oblique and left external oblique are inhibited/lengthened, the torso will bend laterally and rotate to the right.
Training Notes:
- If you have inhibited and excessively lengthened internal obliques, consider the following:
- Increase training volume and training frequency on oblique exercises, as well as abdominal exercises.
- Release and stretch the muscles that are inhibiting the internal obliques, namely the hip flexors and lumbar erectors. Do this on a daily basis.
- Avoid sitting or standing with your lower back excessively arched.
- If lower crossed syndrome is at the root of your inner obliques dysfunction, you need to address it for a complete solution. Refer to my guide on how to fix lower crossed syndrome (article coming soon).
- If you have overactive and short internal obliques, consider the following:
- Reduce training volume and training frequency on oblique exercises.
- Reduce training volume and training frequency on ab exercises that involve bringing your rib cage towards your pelvis.
- Increase training volume and training frequency on lower ab exercises where you pull your pelvis toward your ribs (e.g. reverse crunch), as well as isometric ab exercises (e.g. planks).
- Release and stretch your obliques and upper abs as part of a daily mobility routine.
- Reduce time spent in positions where you’re hunched over.
- Upper crossed syndrome may be causing your inner obliques to be tight. If this is the case, you need to address UCS for a lasting solution. Read how to fix upper crossed syndrome (article coming soon).
- If you have a unilateral dysfunction of the obliques (i.e. same-side internal/external oblique inhibition or overactivity; or internal oblique inhibition on one side with external oblique inhibition on opposite side), consider the following:
- Any of these unilateral dysfunctions may be a sign that some form of scoliosis is present or developing – or they may not be. It could be something completely different, such as a true leg length discrepancy, or simply a muscle imbalance with no bone structure abnormalities involved. If you think you may be developing scoliosis, especially if you’re young, see your doctor to find out.
- You can’t isolate the internal obliques from the external obliques. You simply train the obliques together. As such, I have put the general guidelines and tips for oblique training on one page – see external oblique training notes.

thank you
Great article, I’ve found everything I need to know about my oblique imbalance. Thank you!
Happy to help!
Thank you for the article. It is a true help. I noticed you made reference to writing an article on Lower Cross Syndrome. Is this coming out in the near future?